


Telehealth (or telemedicine) is highly regulated, and as a result, has been difficult to fully adopt. Over the past week, CMS has made changes to broaden access to telehealth services.
Implementing Medicare Telehealth visits allows providers to get reimbursed at the same rate as an E/M visit.
Keep in mind that Telehealth services are available regardless of patient diagnosis; these options are not limited to treating COVID-19.
This guide is targeted at specialists that independently bill for E&M visits, and all information provided below is based on guidance from Medicare and Health and Human Services (HHS). Please consult the full documentation found at the bottom of this page if you choose to act on these recommendations.
Types of Telehealth Services
First, it's important to understand the type of virtual services that exist:
- Medicare telehealth visit
- Virtual check-in
- E-visit
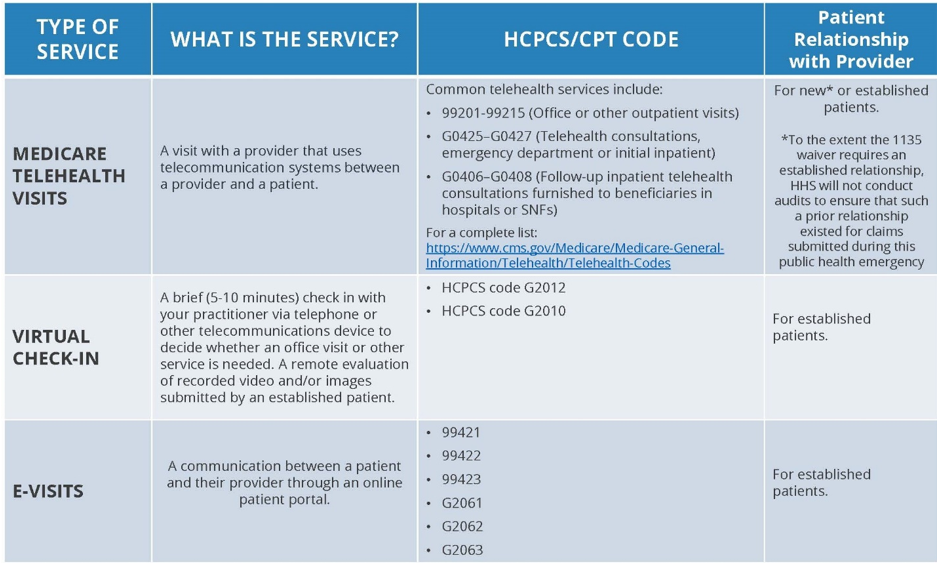
Medicare telehealth visits are an alternative to in-person office visits (synchronous care). You must use both live audio and video except in cases when video conferencing is not available for the patient. Services are billed the same way as they would in your office, and are paid the same as well (for example, E&M codes can be used) using the POS code where the patient would have normally been seen (e.g. clinic facility code). Add the CPT Telehealth 95 modifier to these claims which will indicate the service rendered was performed via telehealth. Telehealth POS code 02 will pay at the traditional telehealth rate, not the in-person rate Medicare has temporarily authorized. Coinsurance and deductible still applies. Eye visit codes 92002, 92012, 92004 and 92014 cannot be used to report telehealth visits.
As of March 30th and until the public health emergency ends, the following changes have been put in place:
- While patients typically need to be in a rural location and at a physical facility, patients can be nationwide, and can be seen from home.
- While patients typically need to have an established relationship with your practice, HHS will not conduct audits to confirm relationship for claims submitted during this time period.
- While it is important to adopt a true telehealth solution, HHS OCR will exercise enforcement discretion and waive penalties for HIPAA violations against health care providers that serve patients in good faith through everyday communication methods such as FaceTime, Skype, Google Hangouts during the public health emergency. More information can be found at the HHS HIPAA Emergency Preparedness site.
- Clinicians should indicate on the claim when they are doing a Telehealth visit at home. They no longer need to update their Medicare Enrollment with their home address.
Virtual check-ins are designed to reduce unnecessary trips to your office. This is available in all areas (not just rural), and do not need to be live (asynchronous care). The patient must have an existing relationship with your practice, and the communication must not be related to an office visit within the previous 7 days and does not lead to an office visit in the next 24 hours (or next available). These services must be patient initiated, but you may need to educate patients on the availability of such service. Coinsurance and deductible still applies; patients must verbally consent to receiving these services.
There is a wide array of methods to conduct virtual check-ins: phone, audio/video, secure text messaging, secure email, or patient portal.
Use HCPCS G2012 when billing for this service and/or G2010 if you are remotely evaluating recorded video and/or images submitted by a patient.
E-visits are non face-to-face communications conducted via a patient portal. This is available in all areas (not just rural), and do not need to be live (asynchronous care). This must be conducted via a patient portal and communications can occur over a 7 day period. The patient must have an existing relationship with your practice. These services must be patient initiated, but you may need to educate patients on the availability of such service. Coinsurance and deductible still applies; patients must verbally consent to receiving these services.
Billing varies based on time:
- 99421: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 5–10 minutes.
- 99422: Online digital evaluation and management service, for an established patient, for up to 7 days cumulative time during the 7 days; 11– 20 minutes.
- 99423: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 21 or more minutes.
How to start offering telehealth services
We typically take the time to fully vet all products and services that we recommend. However due to the urgent nature of this, keep in mind that we have not done our usual evaluation on the products suggested below.- Due to the relaxed policies around HIPAA, you may start by using commercially available technology like Facetime, Hangouts, Skype, etc for Medicare Telehealth Visits. For a better long term solution, consider
- Furthermore, some EHRs are offering reduced cost services for telehealth during this emergency such as Nextech and Modernizing Medicine.
- For Virtual Check-ins and E-visits, we highly suggest using your patient portal. If you do not have a portal, or you are looking for a better option, check out Klara. If you are interested in signing up for an alternative like Klara or you need help getting your current portal up and running, contact us.
Additional resources:
- Medicare Telemedicine Health Care Provider Fact Sheet
- Medicare Telehealth FAQs
- American Academy of Ophthalmology Coding Guide
- CMS Flexibilities in response to COVID-19

